You are viewing 1 of your 1 free articles. For unlimited access take a risk-free trial
Training for longevity: is more always better?

Sports Performance Bulletin looks at new evidence suggesting that excessively high training loads could be detrimental for long-term athlete health
While there’s much debate in many areas of sport and exercise science, one topic that scientists all agree on is the relationship between exercise and health. Over the past 40 years, a huge body of evidence has accumulated showing that regular physical activity is essential for health and well being, and that physical inactivity is a high-risk factor for major disease morbidity – ie an early cause of death(1).The protective power of physical exercise is very significant; a large-scale, prospective study demonstrated that just 30 minutes per day of light-intensity physical activity (eg walking), which replaces sitting for the same duration, is able to reduce the mortality risk from cardiovascular disease by a whopping 24%(2). Moreover, according to the World Health Organisation, regular physical exercise produces multiple health benefits leading to greater longevity and a healthier life, including reduced high blood pressure, improved weight management, a reduction in the risk of type-2 diabetes, and a lower incidence of strokes, heart disease, and various cancers(3).
Gentle, moderate or vigorous?
In an effort to improve health and longevity, health professionals traditionally advised British and American adults to ‘accumulate at least 30 minutes of moderate activity on five or more days of the week’(4,5). These physical fitness guidelines endorsed aerobic exercise, but a greater emphasis was placed on moderate-intensity training in the belief that high-intensity exercise was accompanied by greater risk of adverse cardiovascular events and muscle/joint/tendon injuries and that low- to moderate-intensity activities were more likely to be continued than high-intensity activities(6).However, this advice subsequently came under scrutiny as evidence suggested that more vigorous exercise was more likely to produce tangible health and longevity effects that gentle-moderate intensity. For example, in a large and rigorous study of 44,500 health professionals aged 40–75 years, researchers found that coronary heart disease (CHD) risk was reduced by 18% in those who walked 30 minutes per day but was reduced by 42% in those who ran for one hour per week(7). Men who consistently engaged in any form of vigorous exercise enjoyed a 30% reduction in CHD risk compared to men who maintained a gentle level of exercise. Also, men who increased their exercise intensity from low to vigorous enjoyed an additional 12% reduction in CHD risk. For a more in-depth discussion of exercise intensity and health benefits, readers are directed to Dr Gary O’Donovan’s excellent article.
How much exercise for longevity?
Surprisingly, despite a large body of research into the health benefits of exercise (and its intensity), the ideal dose of exercise for maximum health benefits and longevity remains unknown. Data shows that at least half of Americans are not meeting the physical activity guidelines recommendations of more than 150 minutes per week of moderate exercise(8), while at other end of the spectrum, about 2.5% of U.S. adults may be overdoing exercise, thereby exposing themselves to potential deleterious health outcomes(9).Currently, the ideal dose of exercise for conferring robust health and optimal longevity is being hotly debated in the scientific literature. But a recent study by US scientists looking into training volumes and longevity provides a valuable insight, indicating that more training might not always been better(10). The premise of the study was that previous research back in 1986 had reported a ‘reverse J-shaped’ association between exercise (walking, stair climbing, and sports play) and all-cause mortality(11). This 1986 data found increasing volumes of training produced steadily lower death rates as energy expended on physical activity increased from under 500kcals per week to 3,500kcals per week. Interestingly however, those who expended 3000-3500kcals per week during exercise experienced the largest mortality reduction (54%) whereas those who expended more than 3500kcals per day experienced a lower reduction in mortality (38%) – ie were less protected.
The reverse J-shaped curve
The findings above (and others) prompted the US researchers to look at data on training loads and the incidence of premature deaths caused by cardiovascular disease – the leading cause of early death in Western countries(12). To do this, the researchers pooled the data from nine previous large studies on cardiovascular-related mortality. As figure 1 shows, nearly all of these large observational studies reproduced this reverse J-curve. In this relationship, the risks of cardiovascular disease and premature mortality decline in a dose-dependent fashion – ie larger training volumes result in lower mortality. However, a threshold of exercise is reached at which point the benefits are attenuated compared to less extreme doses of physical activity – ie mortality begins to rise again.Figure 1: All-cause mortality, training loads and incident cardiovascular diseases(10)
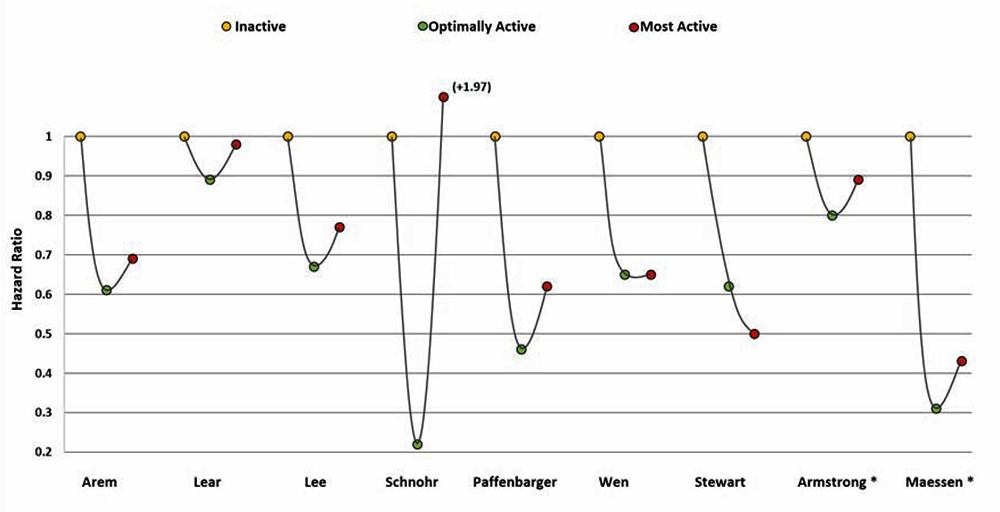
Yellow = inactive; green = optimally active; red = most active
The researchers looked at data for three types of cardiovascular disease in these athletes: coronary artery calcification, myocardial fibrosis and arrhythmias. It was not possible to draw a direct correlation between these types of disease and the occurrence of early death in the athletes. However, the incidence of sudden cardiac death (where no obvious signs of cardiovascular disease are present) was notably higher in athletes undertaking high training loads such as marathon runners and triathletes. This is perhaps not surprising as research shows that longer and more physically demanding events appear to pose a higher risk for sudden cardiac death; data from almost 11 million long distance race participants showed a 3 to 4-fold higher incidence of sudden cardiac death in marathons (1.01/100,000) compared to half marathons (0.27/100,000), with only 29% of victims surviving the cardiac arrest(13). Also, endurance events including marathons and ultra-marathons have been associated with derangements in cardiac biomarkers.
Implications for athletes and trainers
Most athletes don’t train for exclusively for health benefits – they train to win, or at least attain maximal performance and set a new PB. However, for some older athletes, maximizing long-term health through exercise is an extremely important motivating factor when considering training loads. Moreover, some of you reading this may be involved in a coaching or training capacity, and have novice or recreational athletes in your care whose main concern IS maximizing health – for example, those with a prior history of cardiovascular disease.What this data indicates is that where long-term health is a major or prime reason for training, more is not necessarily better, and may in fact be worse. In particular, it seems that very high doses of strenuous exercise may attenuate some of the benefits bestowed by less extreme efforts. From their data above, the research concluded that while the optimal dose of exercise for health remains unknown and probably differs among individuals, current studies suggest that around five hours per week of moderate or vigorous physical activity will confer maximal health benefits. Conversely, training loads significantly above ten hours per week may reduce these health benefits.
However, the researchers were also at pains to point out that the current body of data is not strong enough to recommend that recreational athletes reduce their exercise dose if this is something that improves their quality of life, or is needed to optimize performance in competitions. This is because the risks of higher training loads appear to be somewhat uncertain and modest, especially in athletes with a long training history. Conversely, athletes and coaches should also be aware that if the goal is attain maximum health benefits from exercise, the maximal benefit for CVD risk reduction occurs at much lower, safer and more moderate exercise doses.
References
- Lancet. 2012 Jul 21; 380(9838):247-57
- Clin Epidemiol. 2018; 10():179-186
- World Health Organization: ‘Physical Activity’. (accessed 4th Nov 2020); Available online: www.who.int/news-room/fact-sheets/detail/physical-activity
- JAMA. 1995;273:402-7
- webarchive.nationalarchives.gov.uk/20121102231648/www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4080981.pdf
- Med Sci Sports Exerc. 1998;30:975-991
- JAMA. 1989;262:2395-2401
- Lancet. 2011 Oct 1; 378(9798):1244-53
- Mo Med. 2018 Mar-Apr; 115(2):98-105
- Mo Med. 2020 Jul-Aug; 117(4): 355–361
- N Engl J Med. 1986 Mar 6; 314(10):605-13
- CDC National Health Report Highlights - www.cdc.gov/healthreport/publications/compendium.pdf
- Clin J Sport Med. 2013 Sep; 23(5):409-10
Read More

Related Files

Andrew Hamilton

Latest Issue

Subscribe Today

Newsletter Sign Up
Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up

Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue

Keep up with latest sports science research and apply it to maximize performance
Today you have the chance to join a group of athletes, and sports coaches/trainers who all have something special in common...
They use the latest research to improve performance for themselves and their clients - both athletes and sports teams - with help from global specialists in the fields of sports science, sports medicine and sports psychology.
They do this by reading Sports Performance Bulletin, an easy-to-digest but serious-minded journal dedicated to high performance sports. SPB offers a wealth of information and insight into the latest research, in an easily-accessible and understood format, along with a wealth of practical recommendations.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Performance Bulletin helps dedicated endurance athletes improve their performance. Sense-checking the latest sports science research, and sourcing evidence and case studies to support findings, Sports Performance Bulletin turns proven insights into easily digestible practical advice. Supporting athletes, coaches and professionals who wish to ensure their guidance and programmes are kept right up to date and based on credible science.