You are viewing 1 of your 1 free articles. For unlimited access take a risk-free trial
Overcoming muscle fatigue and sports psychology barriers when competing in a triathlon
Overcoming muscle fatigue and sports psychology barriers when competing in a triathlon
Article at a glanceThe phenomenon of inspiratory muscle fatigue and its impact on athletic performance is explained;
Explanations are provided as to why this fatigue is so detrimental for triathletes, particularly during the cycle-run transition;
Strategies are outlined to help minimise the impact of inspiratory muscle fatigue and so maximise triathlon performance.
The cycle-run transition in triathlon represents a huge psychological barrier for most triathletes, but the perception that running is much harder after cycling is more than just the mind playing tricks. As Alison McConnell explains, the cycle phase presents some serious physiological challenges that triathletes have to overcome as they begin their run
In triathlon, the cycle-run (CR) transition is associated with a number of changes, including an impairment in running economy; specifically, there is a 2-12%(1) decrease in running economy during the early part of the run phase (when compared to running economy in the ‘fresh’ state). The most obvious external cause for this deterioration is a change in running mechanics, which is often apparent as a slightly forward leaning posture. It is thought that this abnormal posture, and the perception of poor coordination after the CR transition may be due to the inability of the neuro-sensory system to adjust quickly to the sudden change of posture from cycling to running. However, there are also some less obvious, and more fundamental physiological changes induced by the cycle phase. The fact that breathing discomfort also seems to be elevated during the early stages of the run phase provides some clues about the origin of these physiological changes.
During triathlon, the lungs are subjected to huge demands, and there have been repeated observations of reductions in post-event lung function(2). An important deficit is that of the lung diffusing capacity, which is impaired post-event(3) (and presumably also during the latter stages of the race). Other respiratory-related changes are also present; specifically, some breathing pump muscles exhibit evidence of fatigue during and after the event. However, the pattern of the changes is not as you might predict.
Research on swimmers has shown that front-crawl swimming is associated with the highest magnitude of inspiratory muscles fatigue (IMF) yet recorded – a 29% deficit in strength after a 200m swim at 90-95% of race pace(4). In light of this, we might predict that IMF would be present after the swim phase of the triathlon and that it would become progressively more severe after the cycle and run phases.
However, the two studies that have examined the influence of triathlon upon respiratory muscle function have shown little or no IMF after the swim phase(2,5). In contrast, both of these studies observed IMF after the cycle and run phases (~25%), but there was no worsening of fatigue between the cycle and run phases. In other words, cycling induced fatigue that was not exacerbated by the subsequent run. In addition, there was no evidence of expiratory muscle fatigue(2).
It is likely that the absence of IMF following the swim phase is due to triathletes’ pacing strategy, and not to the fact that triathletes are more resistant to the IMF induced by swimming than swimmers are. There is some evidence to support this. For example, one study found that the slowest 50% of swimmers were significantly faster in the initial stages of the subsequent cycle phase(6).
Another found that athletes undertaking the swim phase at 80% of their maximal swim trial velocity completed a simulated event faster than when the swim was undertaken at 100% of maximal swim trial velocity. Thus, triathletes probably pace themselves during the swim in the knowledge that not pushing too hard during this phase results in a better overall performance.
It is clear from the data relating to inspiratory muscle fatigue that the cycle phase must represent a particular challenge to the inspiratory muscles, since this phase induces IMF that is not worsened by subsequent running. So what is known about the demands of cycling and the CR transition?
Jargonbuster
Running economy
The energetic cost of running. A reduction in running economy equates to a reduction in efficiency and an increase in the energy requirement for a given pace
Lung diffusing capacity
The ability of the lung to transfer oxygen from the air into the blood
Tidal volume
The total volume of air inhaled/exhaled per breath
Force-velocity relationship
Muscles are able to shorten faster when they are unloaded than when they are loaded and the heavier the load, the slower the maximal velocity of shortening. Every muscle has a maximal velocity of shortening for a given load, which means that every load can represent a maximal load if it is moved at the muscles’ maximal velocity. Thus, moderately loaded movements undertaken as rapidly as possible can be more fatiguing than heavily loaded movements undertaken at slower than maximal velocity.
The cycle-run transition
The CR transition became a particular focus of respiratory research because for many years there was no satisfactory explanation for the increased perception of breathing discomfort that is present during the first minutes of the run phase. As mentioned previously, research has now shown that during the first minute of the run phase following the CR transition, the energetic cost of running is higher. Associated with this is an increase in the ventilatory requirement, and these changes have been ascribed, at least in part, to IMF(7,8).
A research group in France has attempted to tease out the independent and combined influences of cycling and running upon IMF and lung diffusing capacity. In one study(9) they compared the influence of a 20-minute cycle followed by a 20-minute run (CR), with that of a 20-minute run followed by a 20-minute cycle (RC) (all at 75% of maximal oxygen uptake). They found that the RC combination induced the greatest magnitude of IMF. The explanation for this is that cycling presents the greatest challenge to the inspiratory muscles and that when the run follows the cycle, the inspiratory muscles have time to recover. In contrast, when the cycle follows the run, the full magnitude of the cycle-induced IMF is apparent.
But why should cycling be more challenging for the inspiratory muscles than running? It probably relates to the influence of trunk posture upon breathing mechanics. The crouched body position associated with the use of ‘aerobars’ has some disadvantages when it comes to breathing. Research suggests that cyclists who are inexperienced in the use of aerobars experience detrimental effects on their breathing and mechanical efficiency compared to cycling in the upright position(10).
For example, compared with upright cycling, aerobars resulted in a lower maximal oxygen uptake and lower maximal ventilation. In addition, breathing appeared to be constrained, such that tidal volume was lower and breathing frequency was higher. This is a very inefficient breathing pattern; indeed, the study found that mechanical efficiency was lower when using aerobars, ie the same amount of cycling work required more energy.
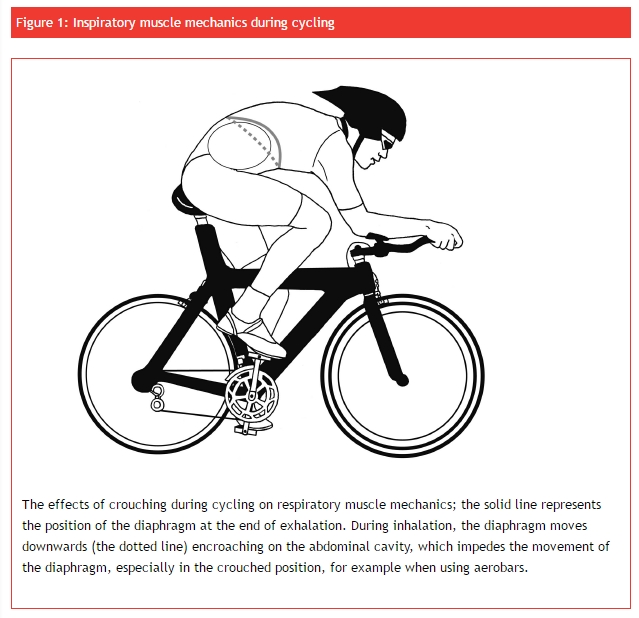
The explanation for these findings resides in the influence of a crouched body position upon inspiratory muscle mechanics during cycling. Firstly, crouching forward forces the contents of the abdomen (stomach, liver and gut) upward against the diaphragm. This impedes the movement of the diaphragm during inhalation because the abdominal contents are pushed up against the diaphragm causing it to ‘work harder’ for each breath (see figure 1). Secondly, the higher breathing frequency means that inspiratory flow rate must be higher, which means that the inspiratory muscles must work in a region of their force-velocity relationship where fatigue and effort sensations are greater.
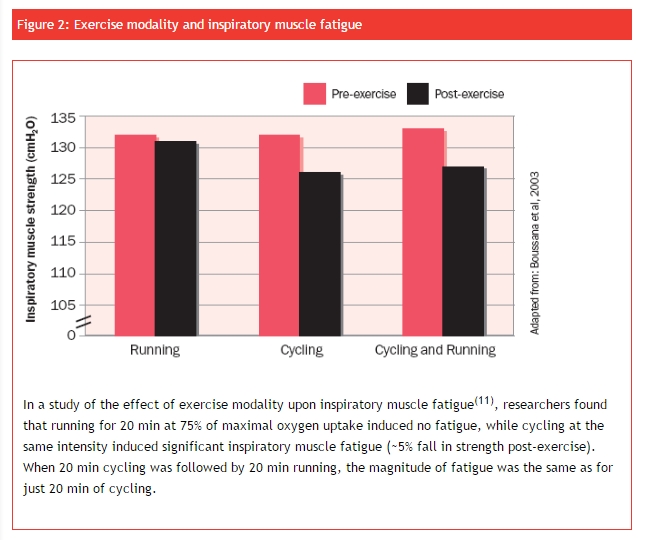
In a follow-up to their RC/CR study, the French group tested their hypothesis that the crouched body position of cycling, and its negative impact upon respiratory muscle mechanics, might account for the differences between the effects of CR and RC transitions(11). Subjects performed either 20 minutes of cycling, 20 minutes of running, or 20 minutes of cycling followed by 20 minutes of running (CR). Interestingly, they noted that cycling and CR induced almost identical IMF, whereas running induced none (see figure 2). This suggests that cycling fatigues the inspiratory muscles in a unique way that is most likely related to the crouched body position.
As mentioned above, changes in lung diffusing capacity have also been noted after CR and RC transitions(12). As was the case with IMF, the RC transition generated the greatest deficits in diffusing capacity. The authors speculated that this was due to a reduction in the volume of blood within the lung circulation during RC, which would reduce the proportion of the lung available for oxygen exchange between blood and air. Further, they speculated that the reduced lung blood volume was due to IMF, and secondary to alterations in breathing-induced pressure changes within the chest and thus to the amount of blood returning to the lungs.
Another potential explanation for the change in diffusing capacity relates to the influence of IMF upon blood flow distribution during exercise. During exercise that fatigues the inspiratory muscles, there is a narrowing of blood vessels, including those to working muscles(13), and possibly also those in the lungs.
A recent study into the influence of inspiratory muscle training (IMT) on exercise performance under conditions of simulated high altitude (low oxygen) using a PowerBreathe training device found that oxygen diffusing capacity and arterial oxygen saturation were increased during exercise after IMT, compared to before IMT. This may indicate that after IMT, a vasoconstrictor influence upon the blood circulation to the lungs has been removed, causing blood volume and diffusing area to be increased. Thus, the impairment of diffusing capacity at the CR transition of the triathlon may be a manifestation of pulmonary vasoconstriction that has been induced by inspiratory muscle fatigue.
It seems likely therefore that the respiratory impairments induced by cycling carry over into the run, causing run performance to also be impaired. The greater IMF induced by the RC combination most likely occurs because in the CR combination, the inspiratory muscles can recover slightly from the impairments induced by the preceding cycle; whereas in the RC combination, there’s no opportunity for recovery. It appears that the mechanical constraints of cycling, which restrict rib cage and diaphragm movement, induce impairments in both inspiratory muscle function and lung diffusing capacity, both of which can impair performance.
Overcoming IMF
The obvious question is what can be done to minimise these effects? Since studies appear to show that the aerobar position has fewer detrimental effects in cyclists who have used them for a prolonged period(10), it appears likely that the inspiratory muscles adapt to the increased demands imposed by aerobars. Clearly this adaptation doesn’t appear to abolish the IMF, since there are numerous studies showing that even very highly trained triathletes and cyclists still experience IMF. However, an intervention that has been shown to abolish IMF is specific resistance training of the inspiratory muscles(14).
The benefits of inspiratory muscle training
“Something that sets professional cyclists apart from mere mortals is the fact that their breathing remains deep and strong throughout intense exercise, maximising efficiency and minimising the metabolic cost of breathing”
The data described above creates a fairly compelling argument in favour of specific inspiratory muscle training (IMT) in order to minimise the detrimental influence of the mechanical constraints to breathing that are imposed by cycling. Unfortunately, there are so far no published studies evaluating the benefits of IMT for triathlon performance. However, we can infer the likely benefits by considering the following facts, as well as data from studies of IMT in cyclists, all of which suggest that good breathing and avoiding IMF are central to success:
All three disciplines of the triathlon elicit inspiratory muscle fatigue (IMF) when undertaken individually;
IMT improves performance in both cycling(15) and running(16);
The cycle-run component of the triathlon is associated with IMF, as in the event as a whole(2,5);
Inexperienced cyclists using aerobars experience detrimental effects on their breathing and a decrease in mechanical efficiency compared to cycling in the upright position(10);
Something that sets professional cyclists apart from mere mortals is the fact that their breathing remains deep and strong throughout intense exercise, maximising efficiency and minimising the metabolic cost of breathing(17).
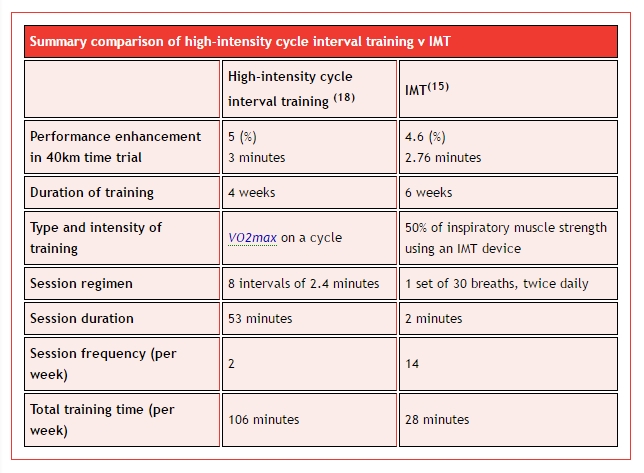
Finally, in considering the merits of adding IMT to an already time-consuming training schedule, it’s worth considering some facts regarding the time efficiency of IMT compared other training adjuncts. A typical IMT programme requires less, around 4 minutes per day, and can produce a 4.6% improvement in 40km cycling time trial performance(15). So let’s consider what else could be added to a training schedule in order to achieve a similar magnitude of benefit.
Very few studies have examined the influence of adding a different type of training to the endurance regimens of already highly trained endurance athletes. Fortunately, one of the few studies to have undertaken such an appraisal utilised a 40km cycling time trial as an outcome measure, making it possible to compare their data directly with those obtained using IMT.
The authors examined the effect of a number of interval training regimens, one of which produced an improvement in 40km time trial performance of ~5% over the 4-week period of their training intervention(18). The intensity of training was very high, being set at the power output that elicited maximal oxygen uptake (VO2max) during an incremental exercise test. Athletes were required to undertake eight intervals of ~2.4 minutes duration interspersed with recovery periods of ~4.8 minutes. Athletes trained twice per week and the duration of each session was ~53mins.
Over the 4 weeks of the intervention, the total duration of high-intensity interval training required to elicit a 5% increase in 40km time trial performance was 7hrs. Compare this to the total time required to attain a 4.6% improvement in performance following 6 weeks of IMT, which is around 1.8hrs! Another salient point is the intensity and duration of each training session (53 minutes at VO2max v 2 minutes at moderate inspiratory muscle load), as well as the fact that IMT can be undertaken anywhere; there’s no need for a bike, or even to break into a sweat! The choice is yours…
Summary
In this article we have considered the unique challenge to breathing posed by the triathlon, as well as the rationale for training the breathing pump muscles. Inspiratory muscle fatigue appears to contribute to the discomfort and physiological challenge of the run phase of triathlon. However, IMT reduces this fatigue and improves cycle time trial performance, indicating a strong likelihood that it will also ease the CR transition in triathlon, thereby enhancing performance. We’ve also considered what else could be added to a training programme to obtain the same performance improvement that has been demonstrated in response to IMT. The numbers speak for themselves and make the argument in favour of IMT a complete ‘no brainer’. It’s quick, it’s easy, it’s convenient, and you don’t need to flog your guts out. Just add 4 minutes per day of relatively easy exercise to your normal training to achieve a 4.6% gain in your 40km time trial performance!
Alison McConnell is currently professor of applied physiology at Brunel University; her research interests are in respiratory limitations to exercise performance.
References:
Br J Sports Med 2000; 34:384-90
Med Sci Sports Exerc 1991; 23:1260-4
J Sports Med Phys Fitness 2001; 41:441-7
J Sports Sci 2003; 21:659-64
J Physiol 1996; 165P
Int J Sports Med 2006; 27:43-8
Eur J Appl Physiol Occup Physiol 1998; 77:98-105
Med Sci Sports Exerc 1999; 31:1422-8
Med Sci Sports Exerc 2001; 33:2036-43
Br J Sports Med 37 2003; 441-4
Int J Sports Med 24 2003; 63-70
Eur J Appl Physiol 90 2003; 489-95
Respir Physiol Neurobiol 2006; 151:242-50
Med Sci Sports Exerc 2002; 34:785-92
J Sports Sci 2002; 20:547-62
Eur J Appl Physiol 2004; 93:139-44
Sports Med 35 2005; 285-312
Med Sci Sports Exerc 2002; 34:1801-7

Andrew Hamilton

Latest Issue

Subscribe Today

Newsletter Sign Up
Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up

Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue

Keep up with latest sports science research and apply it to maximize performance
Today you have the chance to join a group of athletes, and sports coaches/trainers who all have something special in common...
They use the latest research to improve performance for themselves and their clients - both athletes and sports teams - with help from global specialists in the fields of sports science, sports medicine and sports psychology.
They do this by reading Sports Performance Bulletin, an easy-to-digest but serious-minded journal dedicated to high performance sports. SPB offers a wealth of information and insight into the latest research, in an easily-accessible and understood format, along with a wealth of practical recommendations.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Performance Bulletin helps dedicated endurance athletes improve their performance. Sense-checking the latest sports science research, and sourcing evidence and case studies to support findings, Sports Performance Bulletin turns proven insights into easily digestible practical advice. Supporting athletes, coaches and professionals who wish to ensure their guidance and programmes are kept right up to date and based on credible science.