Frozen shoulder: a sticky problem

SPB looks at an injury condition known as ‘frozen shoulder’, and the best treatment options for restoring shoulder functionality
Frozen shoulder, more correctly known as adhesive capsulitis (AC), is a common cause of shoulder pain and loss of shoulder joint motion in the over 40s. In ‘primary’ cases of AC, there is no significant reason for the onset pain or stiffness, whereas secondary AC can occur following an injury, trauma, surgery or illness. In younger people below the age of 40 and athletes, primary AC is rare; AC is more likely to be secondary in nature – for example following a rotator cuff injury. When AC does occur however, it can result in considerable disruption to any sports activity, especially given the typically long timescale it requires to resolve. Indeed, as the author of this article, I can personally testify this fact. Following a violent wrench to the left arm and shoulder when our greyhound accelerated full pelt after a rabbit while on the leash, I suffered a 21-month period of AC injury during which my usual sporting activity was severely curtailed!What causes AC?
As its terminology implies, adhesive capsulitis describes a condition where the shoulder joint capsule becomes inflamed and ‘sticky’ (see figure 1), making the whole joint stiff and difficult/painful to move. The cause of AC is poorly understood. We do know however that as the capsule becomes inflamed, scar tissue forms, which causes pain and leaves less room for the humerus (upper arm bone) to move through its normal range of motion (see figure 1).Figure 1: schematic representation of AC
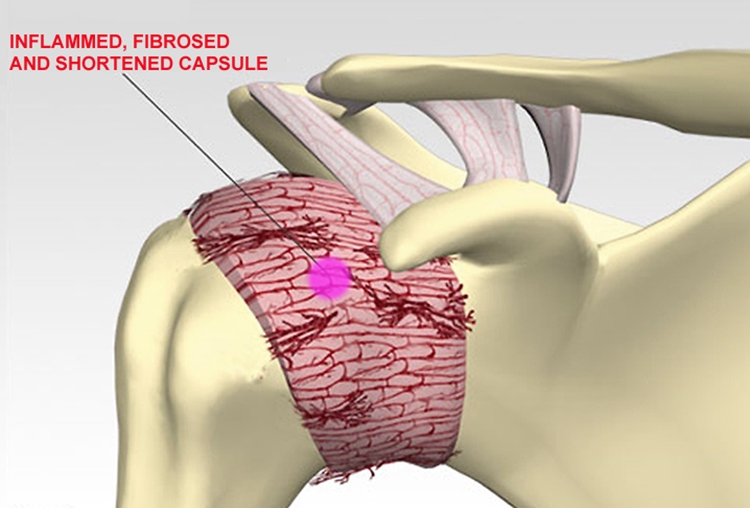
The joint capsule shortens as inflammation progresses, restricting humerus range of movement.
Tissue sampling from patients with AC suggests a proliferative mechanism for the condition where the individual fibres of the capsule become progressively affected(1). Meanwhile on a bigger scale, there is thickening and shrinking of the front of the shoulder capsule, leading to reduced shoulder joint volume, and shoulder range of motion (ROM) - particularly external rotation with the arm moderately elevated (see figure 2)(2). Other studies have suggested a link between the risk of AC and some metabolic conditions such as diabetes and raised blood lipids such as cholesterol and triglycerides(3,4).
Figure 2: External and internal rotation
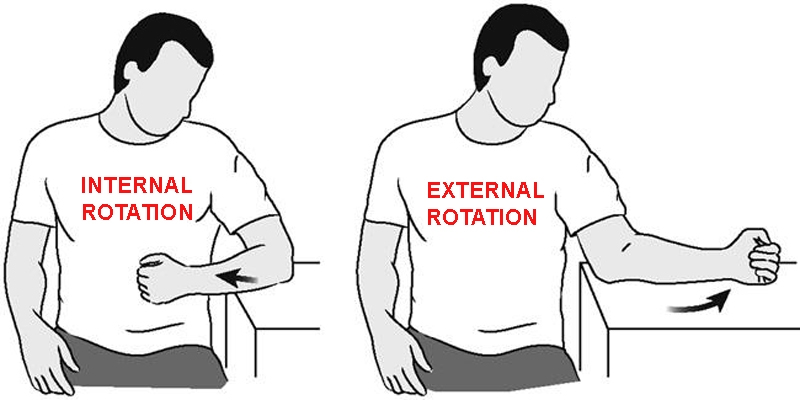
In AC, pain and restricted movement particularly affects external rotation movements of the arm.
From an athlete’s perspective, there’s some evidence that shortening of one or more of the ligaments of the shoulder (eg through poor posture) may also increase the risk of AC. Therefore, athletes whose training results in overdeveloped and/or shortened chest of frontal shoulder muscles (eg swimmers, boxers, throwing athletes) may be at increased risk(5). Also, prolonged immobility (for example after a rotator cuff injury or shoulder fracture) is known to be a risk factor for AC – a good reason for all athletes to rehab a shoulder injury as rapidly as possible! Despite all of these risk factors however, in many primary cases of AC there is absolutely no identifiable cause, something that can be very frustrating for clinicians and sufferers alike.
AC characteristics
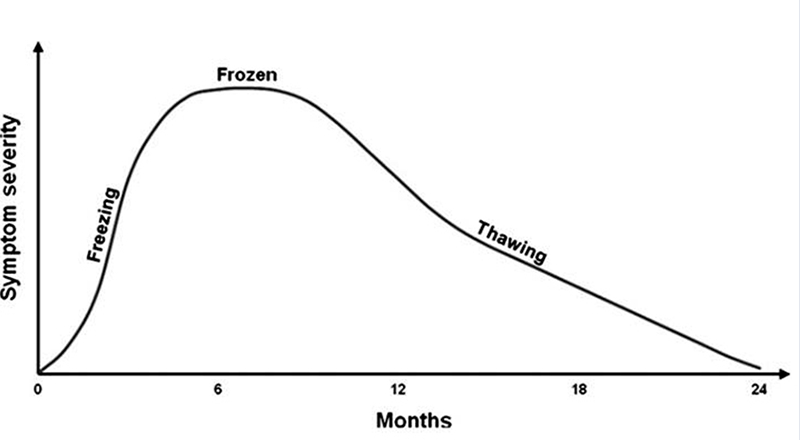
AC typically displays a progression through three distinct phases: freezing, frozen and thawing (schematically represented in figure 3):- In the initial phase (freezing), patients typically suffer with a marked pain that comes on over a period of a few weeks with activity. At this point however, there is no noticeable loss of range of movement.
- The frozen (adhesive) phase typically lasts for 3-9 months, with significant stiffness and pain at the extremes of movement. Patients presenting in this phase often hold the arm close to the body (in adduction) and with internal rotation to reduce pain. There is usually a global (and painful) restriction of shoulder movement, with almost complete loss of external rotation.
- The thawing (resolution) phase typically lasts for 9-18 months, and is characterized by steadily diminishing levels of pain and stiffness. However, the improvements are only slow and it may significantly longer for complete thawing to occur, with some studies suggesting a timeframe of up to 3-10 years(6-9).
Figure 3: Schematic representation of typical time course and symptom severity in AC
Diagnosis
AC can be difficult to diagnose in its early stages and to differentiate from other common shoulder disorders. However, in addition to the clinical features described above (in particular the almost complete loss of external rotation), the typical pattern of AC onset as described above is also helpful in making a diagnosis. Caution is needed however; while the consensus view is that a diagnosis of AC can usually be confirmed by a sports physiotherapist in the clinic(10), some research suggests these typical signs and symptoms during onset may not be experienced by all patients(11).In cases where there is doubt about whether an athlete’s shoulder injury is a case of AC, he or she should be referred for MRI imaging. If the scan shows a thickening in the joint capsule and the affected ligaments, this will provide strong evidence for AC(12,13). Indeed, recent evidence demonstrates MRI scans can detect distinct physical changes in the shoulder tissues associated with the freezing, frozen and thawing phases of AC(14). By contrast, routine X-rays for a case of suspected frozen shoulder is not recommended. This is because the evidence suggests that X-ray imaging offers little extra information over and above a diagnosis made by a sports physician based on the athlete’s history and clinical examination alone(15).
Treatment options
The use of non-steroidal anti-inflammatory medication (NSAIDs – eg Ibuprofen) can help provide some symptomatic relief of AC, but there’s little evidence these medications can ameliorate the disease progression. Physiotherapy on the other hand may be rather more successful; studies examining the role of physiotherapy in the early and mid-stages of AC have shown an improvement in pain scores, functionality and range of motion(16-22). In prolonged cases that refuse to resolve, with conservative treatment options, surgery or injections may be recommended, particularly in second and third phases of AC. The most common approaches are as follows(23):- Manipulation under anaesthesia (MUA), where the shoulder capsule is manually stretched while the patient is under anaesthetic (to avoid excessive pain).
- Arthroscopic capsular release, where an incision of the capsule is made to loosen the tissue and free up movement.
- Injections into the shoulder capsule to relax the tissue and reduce the fibrous-induced ‘stickiness’.
Physio vs. manual therapy vs. injections
The best treatment route for AC remains a hot topic of debate – perhaps unsurprising given the cause of AC is still poorly understood. For example, some research suggests that patients receiving physiotherapy alone have better clinical outcomes than patients undergoing MUA(17), whereas other research suggests that ‘supervised neglect’ – ie doing pretty much nothing – may provide a better outcomes at two years than an intensive physiotherapy regime(24)! The efficacy of MUA is also far from clear; one recent study concluded that there’s actually not enough evidence to recommend it for patients(25).A 2014 review study investigated the effectiveness of physiotherapy and exercise – in particular, how it compared to steroid injections(26). Analysing data from 32 randomised controlled trials, it concluded that: using a combination of physiotherapy and exercise to combat AC may be less effective than simply giving a steroid injection – at least in the short term. These findings were echoed by an earlier meta-review (a study that pools data from a number of previous studies), which compared(27):
- Steroid injections
- Sodium hyaluronate injection (based on hyaluronic acid – a natural joint lubricant)
- Supervised neglect (doing nothing)
- Physical therapy (mainly physiotherapy exercises)
- Acupuncture
- MUA
- Distension and capsular release (manipulation to stretch the joint capsule)
Stretching success
For athletes trying to recover from AC, or clinicians trying to treat them, the findings above are somewhat discouraging. However, conservative and easily implemented approach that may be of value is the use of stretching. A study by Indian researchers looked at the effectiveness of sustained stretching of the shoulder capsule on range of movement, pain, and function in patients with a frozen shoulder(28). This study took 100 patients and compared 20 minutes a day for five days per week for two weeks of:- Physiotherapy only
- Stretching (using traction) and physiotherapy
Figure 4: Stretching (using countertraction) and improvements in range of movement(28)
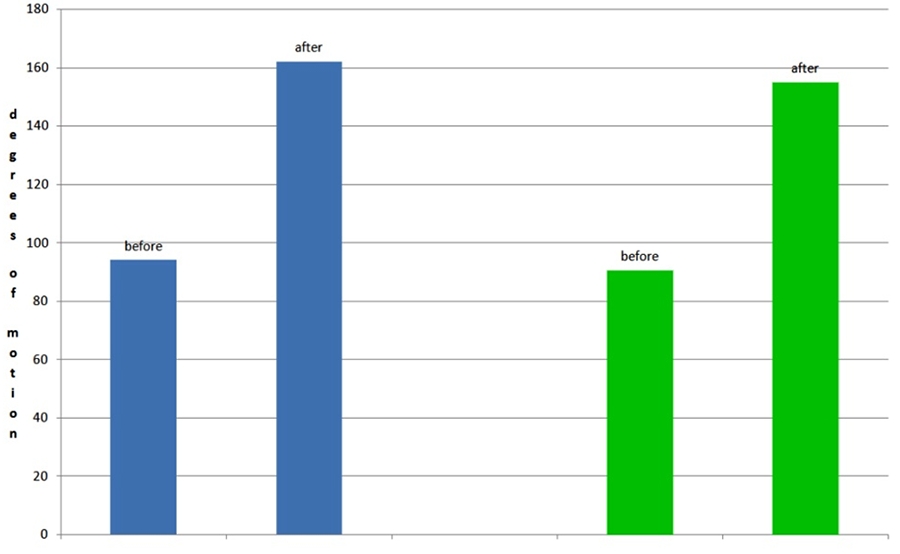
Blue bars show before and after degrees of motion scores for shoulder flexion, while green bars show before/after scores for abduction.
Mulligan’s mobilizations for trainers, masseurs and clinicians
Related to stretching, athlete trainers and sports clinicians/masseurs might be interested in data from another recent study, which looked at the effectiveness of a stretching and mobilisation technique known as Mulligan’s mobilization with movement (MWM) for treating AC(29). Using high-quality data from randomized, controlled trials, the researchers analyzed 18 studies with 753 participants for the effects of MWM on range of movement (ROM). They found that using MWM seemed to produce better therapeutic results in comparison to other passive or active approaches. In particular, shoulder range of movement improved consistently in all movement directions. Those interested in using this approach are directed to the video link shown below, which explains the concept and application of a Mulligan’s mobilization for treating.
High-tech approach?
In recent years, a more high-tech treatment option has become increasingly popular for AC. Extracorporeal shock wave therapy (ESWT) is a non-invasive treatment that uses the mechanical force of a powerful acoustic shock wave (emitted from a wand held on the surface of the skin) within injured tissues in order to reduce pain and speed healing of the affected area. The exact mechanism by which ESWT is able to exert its actions within tissue is not well understood but it is believed that:- ESWT disrupts fibrous tissue allowing for the subsequent promotion of revascularization and healing of tissue.
- The direct and indirect effects of the shock waves impair the transmission of pain signals (allowing the athlete to put the shoulder through a greater range of motion during therapy).
- The high-energy shock waves are able to break up fibrous/calcified deposits, thereby loosening structures within the shoulder capsule.
In summary
Many athletes will never have to endure a frozen shoulder injury in their careers, which is great news. However, when it does occur, it can be a very frustrating and intractable challenge – both for the affected athlete and those trying to treat him/her. Not only are the causes still poorly understood, this condition takes a considerable time to resolve (even in the best-case scenario), and there remains much uncertainty about truly effective conservative treatment approaches. Although physiotherapy and manual therapy should remain the first port of call, the evidence that they speed healing in the longer term is weak. The evidence for steroid injection therapy is somewhat more robust however, and more recent evidence suggests that stretching techniques and Mulligan’s mobilizations could be useful tools in the clinician’s armoury. Another treatment approach worth considering by athletes and clinicians is ESWT, which although harder to obtain and more costly, is supported by good evidence. Above all, athlete patience is the key, along with the knowledge that even the worst cases do resolve in time!References
- J Bone Joint Surg Br. 1995;77(5 ):677
- J Bone Joint Surg Am . 1989 ;1(10 ):1511
- South Med J. 2008 Jun;101(6):591-5
- Rheumatol Int. 2014 Jan;34(1):67-74
- Open Orthopaedics Journal, 2013, 7, (Suppl 3: M10) 352-355
- Br Med J 2005;331(7530): 1453-6
- Curr Rev Musculoskelet Med 2008; 1(3): 180-9
- Br J Gen Pract 2007; 57: 662-7
- Scand J Rheum 1975; 4(4): 193-6
- Open Orthopaedics J, 2013, 7, (Suppl 3: M10) 352-355
- Phys Ther. 2014 Jul;94(7):968-76
- J Bone Joint Surg Br 1995; 77(5): 677
- J Bone Joint Surg Am 1989 ;71(10): 1511
- Indian J Radiol Imaging. 2019 Jan-Mar;29(1):19-24
- Musculoskeletal Care. 2019 Jun;17(2):288-292
- J Bone Joint Surg Am 2000; 82(10): 1398.
- Arch Orthop Traum Surg 1995; 114(2) : 87-91.
- Ann Rheum Dis 1984; 43(3): 353-60.
- Arthritis Rheum 2003; 48(3): 829-38.
- Physiotherapy 2002; 88(8): 450-7.
- Br Med J 1998; 317(7168): 1292-6.
- Cochrane Database Syst Rev 2003;(2): CD004258
- Shoulder Elbow 2010; 2(4): 294-300
- J Shoulder Elbow Surg 2004; 13(5): 499-502
- EFORT Open Rev. 2019 Mar 19;4(3):98-109
- Cochrane Database Syst Rev. 2014 Aug 26;8:CD011275
- Health Technol Assess. 2012;16(11):1-264
- Clin Orthop Relat Res. 2014 Jul;472(7):2262-8.
- J Manipulative Physiol Ther. 2019 Jul 16. pii: S0161-4754(18)30270-7
- J Shoulder Elbow Surg. 2014 Dec;23(12):1843-1851
- Int J Prev Med. 2014 Jul; 5(7): 875–881
- J Phys Ther Sci. 2015 Dec;27(12):3659-61
- J Phys Ther Sci. 2017 Nov; 29(11): 1907–1909
You need to be logged in to continue reading.
Please register for limited access or take a 30-day risk-free trial of Sports Performance Bulletin to experience the full benefits of a subscription. TAKE A RISK-FREE TRIAL
TAKE A RISK-FREE TRIAL

Andrew Hamilton

Latest Issue

Subscribe Today

Newsletter Sign Up
Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up

Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue

Keep up with latest sports science research and apply it to maximize performance
Today you have the chance to join a group of athletes, and sports coaches/trainers who all have something special in common...
They use the latest research to improve performance for themselves and their clients - both athletes and sports teams - with help from global specialists in the fields of sports science, sports medicine and sports psychology.
They do this by reading Sports Performance Bulletin, an easy-to-digest but serious-minded journal dedicated to high performance sports. SPB offers a wealth of information and insight into the latest research, in an easily-accessible and understood format, along with a wealth of practical recommendations.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Performance Bulletin helps dedicated endurance athletes improve their performance. Sense-checking the latest sports science research, and sourcing evidence and case studies to support findings, Sports Performance Bulletin turns proven insights into easily digestible practical advice. Supporting athletes, coaches and professionals who wish to ensure their guidance and programmes are kept right up to date and based on credible science.