You are viewing 1 of your 1 free articles. For unlimited access take a risk-free trial
Body fat measurement: getting to the truth
How reliable are body composition measuring devices, and which methods should athletes and coaches use for monitoring? SPB looks at brand new research

Distinguishing between lean body mass and fat mass is vital for athletes and coaches. While some body fat is essential for good health and physiological function, carrying excess weight in the form of surplus body fat inevitably blunts athletic performance by reducing ‘power-to-weight’ ratio. Unlike muscle, body fat is not involved in energy production and can therefore be considered as ‘deadweight’. Carrying surplus body fat means that the working muscles have to share finite energy production around more lbs of deadweight body mass. This means less power output per kilo of bodyweight overall, and a lower sustainable pace in any sports where gravity is involved. So when athletes say they would like to lose some weight, what they really mean is that they’d like to lose some deadweight, or body fat. The problem however is that accurately distinguishing between lean body mass and fat – ie determining body composition - is actually quite difficult to do.
Body composition analysis
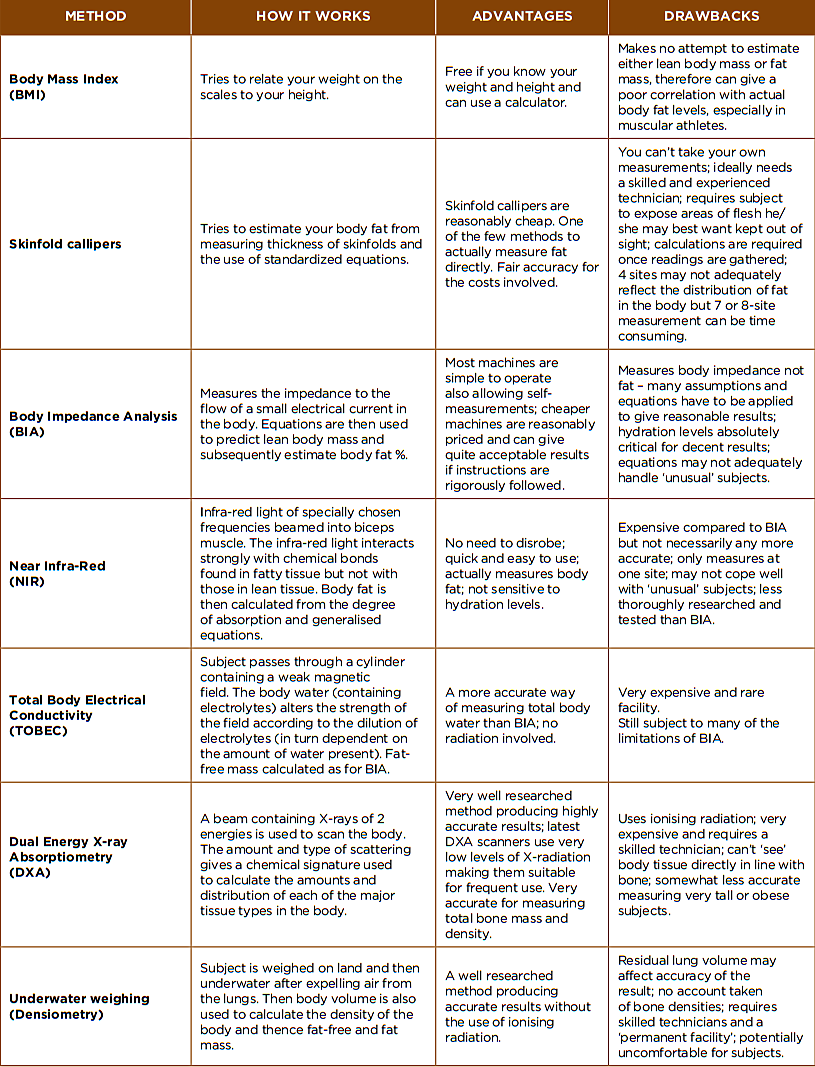
Those of you who are old enough may remember the “Can you pinch an inch?” slogan used in Kellogg’s Special K cereal ads during the 1980s. The slogan implied that being able to pinch an inch thickness of fat around the waist was a good indicator of excessive body fat (a gross oversimplification in fact). In 2026 fortunately, there are far better and more accurate ways to determine your body fat and lean muscle mass content. Table 1 summarizes some of the most common methods currently used in commercial and research settings, and outlines their advantages and drawbacks. The three methods most widely used among athletes and their coaches are:
· Bioelectrical Impedance Analysis
· Skinfold measurements (anthropometry)
· Dual-Energy X-ray Absorptiometry (DXA – used mainly to test pro athletes in a clinical setting)
Of these, DXA is considered the ‘gold standard’. It is highly accurate and can not only determine lean muscle mass and fat mass, but bone mass and bone density too(1,2). The drawback however is that it requires specialized clinical facilities and highly trained technicians to operate the scanner. Although DXA is often used to assess elite athletes (who will have the support of professional teams/bodies), it is quite expensive and often inaccessible for most amateur athletes.
Table 1: Body composition analysis methods
Athlete testing
Because of this, amateur athletes and their coaches often rely on simpler and cheaper body composition analyzers such as those using bioelectrical impedance analysis (BIA – devices that send a small electrical current through the body to measure water content then deduce muscle fat mass using equations) or simple skinfold measurements (which involves measuring skinfold thickness at a number of specific sites using special skinfold calipers then applying standardized equations to calculate fat and lean body mass).
But while these simpler devices can be useful to track body composition changes over time, there is a problem; BIA devices they have been developed for the general (largely sedentary) population rather than for use by endurance athletes such as runners, cyclists and triathletes(3,4). Athletes tend to have much greater variations in hydration status and in skeletal muscle tissue. Meanwhile, skinfold measurements assume a standardized regional distribution of body fat stores tissue, but the distribution in athletes is likely to be significantly different(5,6). Also, skinfold measurements can produce variable results depending on the number and location of sites sampled, the skill of the technician and the equations used(7).
This means that when athletes use BIA and skinfold measurement to assess body composition, there are likely to be significant biases and estimation errors due to differences in body density, water content, and muscle mass. In plain English, body composition analyzers developed for the general public are already subject to a degree of error, but in athletes, these errors may be significantly larger due to differences in hydration, muscle mass, body fat distribution and bone density, which are typically induced about when an athlete undergoes a period of serious training! What would be useful is some data on how BIA and skinfold measurement stack up against each other and how they compare to the gold standard (DXA) when used in trained athletes. Fortunately, we can turn to some new research on triathletes for some answers.
New research
Published in the journal ‘Nutricion Hospitalaria’, this research by a team of Mexican sports scientists sought to discover which of these two commonly used body composition measurements (BIA/skinfold measurement) most closely aligns with the ‘gold standard’ DXA results when used for well-trained triathletes(8) In particular, they wanted to find out what happens when body composition measurements are taken by expert technicians under rigorously controlled conditions – ie with as much user error eliminated as possible.
To do this, the researchers recruited 26 triathletes (18 men and 8 women) with an average age of approximately 34 years. All the triathletes were keen amateurs, training at least five times per week, with at least six months triathlon training background. In a random order, all of the 26 triathletes underwent three types of body composition assessments on the same day. These were as follows:
· DXA scanning – this entailed a full-body scan using a ‘GE Lunar Prodigy densitometer’. This provided accurate data on three types of tissue in the body: bone mineral content, lean mass, and fat mass. The results from this DXA were then used as the reference point.
· BIA – this was carried out using an ‘In-Body 720 multi-frequency analyzer’, which estimated the triathletes’ body water content based on electrical current resistance, which was then used to calculate body fat percentage.
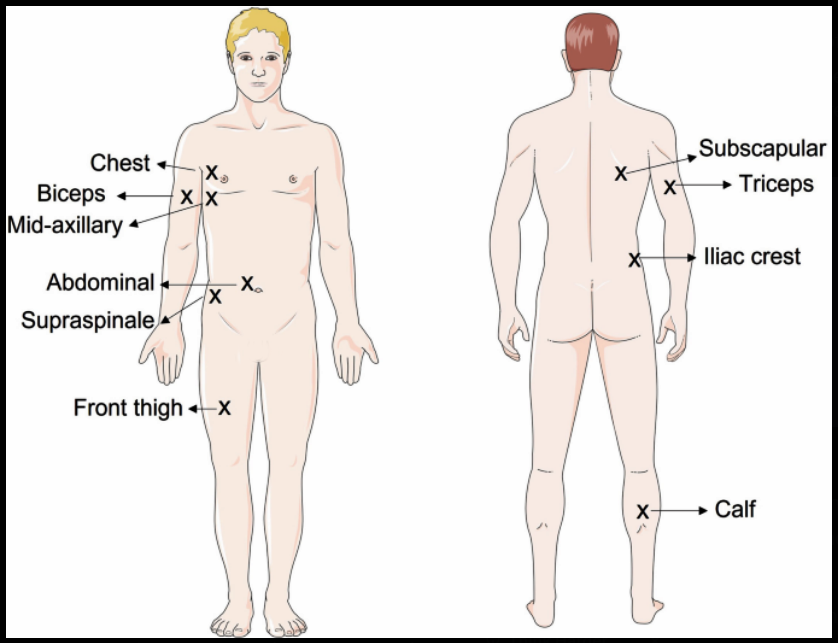
· Skinfold measurements – the researchers measured eight different skinfold sites (triceps, subscapular (just below the shoulder blade), biceps, iliac crest (top of the hip bone, roughly where people place their hands when ‘putting hands on hips)’, supraspinale (side of the torso, in the lower abdominal/upper hip region, slightly above the hip bone), abdominal, front thigh, and the calf - see figure 1. These measurements were taken using a strict protocol set out by the International Society for the Advancement of Kinanthropometry (ISAK) and then used a well-validated mathematical formula known as the ‘Withers equation’, which is frequently used for determining body fat percentage in athletic populations.
To ensure consistency and a fair comparison, all participants observed strict dietary and hydration protocols prior to measurements being taken(9). This involved:
· A minimum of eight hours of fasting prior to testing.
· At least 24 hours without performing physical exercise.
· A minimum of 48 hours without consuming any of alcoholic beverages or any medication that might affect hydration.
· For the female triathletes, the measurements were timed between the follicular phase, ovulatory phase, and up to 7 days before the end of the luteal phase. This was to ensure no fluid-related alterations associated with the menstrual cycle.
Figure 1: Common skinfold sampling sites
All the triathletes were assessed in the morning using all three methods before breakfast and to make doubly sure that hydration levels were in the reference range, the triathletes’ urine specific gravity was tested before any body composition measurements, with values between 1010 and 1020 used to indicate proper and complete hydration(10).
What they found
The first finding was that the three different methods of measuring body composition showed significant differences in the results they produced, highlighting the fact that they are not interchangeable. This means that to track changes in body composition in an athlete, the same method should be used throughout. Just as important were the findings comparing BIA and skinfold measurements to DXA scans (the gold standard reference). On average, BIA method showed a tendency to underestimate body fat percentage, especially in the male triathletes.
To make matters worse, BIA measurements had ‘wide range of error’. In short, there was a lot of ‘spread’ of body fat estimation around the actual fat percentage as determined by DXA. This means that for any individual athlete, while there’s a tendency on average to underestimate body fat, BIA might still report a fat percentage that is significantly higher or lower than the true value, thereby increasing the uncertainty of the result. As the researchers pointed out, this is likely due to the fact that BIA is very sensitive to hydration levels, and the fact that the typical physiological traits of athletes (eg higher total body water and different glycogen storage characteristics) are different to those in sedentary adults.
The skinfold measurements also tended to underestimate body fat percentage compared to DXA, but unlike BIA, there was no significant discrepancy in the results between males and females. More importantly, the skinfold results were more tightly correlated to the DXA results, with a correlation coefficient of 0.876 compared to 0.697 for the BIA results. [NB: the closer a correlation coefficient is to 1.0, the stronger the linear relationship between two variables] This indicates that the skinfold measurements produced around 57% less variance from the true DXA result compared to BIA, showing a much tighter relationship and less likelihood of error compared to DXA. In short, skinfold measurements provided a more reliable and predictable estimate of body fat in triathletes – a finding that aligns with previous research suggesting that manual measurements of subcutaneous fat (ie skinfolds) are often more reliable for lean athletes than BIA(11).
Implications for athletes
What are the main takeaway points from this new research? The first thing to say is that relying on BIA measurements to get accurate body fat percentage measurements is fraught with problems. It’s not just that BIA tends to underestimate fat levels, it’s also that there’s quite a lot of variability, which is likely related to changes in hydration. This variability means that tracking body composition changes over time may also be unreliable due to the inconsistent measurements. This makes it harder for athletes and coaches to monitor small body composition changes through the season – for example when making dietary adjustments designed to reduce body fat. That said, so long as you understand its limitations, BIA still has a place, especially if you are an amateur athlete without access to a coach or technician who can perform skinfold measurements.
The second takeaway is manual skinfold measurements provide a much more consistent reflection of an athlete’s actual fatness (adiposity), and should therefore be considered a superior choice to BIA for coaches tracking their athletes. Skinfold callipers are not fooled by the hydration changes common in endurance athletes! Ideally, the coach or assistant taking skinfold measurements should be well-trained (ideally ISAK certified) to minimize human error. The Withers equation is recommended for calculating actual body fat percentage from skinfolds; however, even without using an equation to get a body fat %, simply adding up the sum of skinfold measurements in millimetres is an excellent way to track body fat gains/losses over a period of time, and avoids any possibility of mathematical errors that can occur when manipulating equations.
Thirdly, whatever method is used, consistency is essential because different methods are likely to produce different numbers. An athlete or his/her coach should never compare a BIA result to a skinfold result or a DXA result from a clinic. If you are tracking changes over time, pick one method and stick to it. If you are an amateur and need to self measure, you will likely still need to use BIA – unless you can get your partner or a friend you trust to undergo some training and take skinfold measurements for you! When using BIA, remember that hydration is critical; try to take the readings at the same time of day (and time of month for women) when fully rested and hydrated. Finally, if you really do want to know your actual body fat levels and body composition, the best option of all is stump up some cash and seek out a DXA scan!
References
1. J Physiol 1996 Dec;271(6 Pt 1):E941-51
2. J Sports Sci 2009 Mar;27(5):469-77
3. Nutr J 2007;15;6(1):18
4. Br J Nutr 1974 Jul;32(1):77-97
5. J Strength Cond Res 2015;29(4):918-25
6. International Standards for Anthropometric Assessment. Esparza-Ros F VCRMJM, editor. 2019
7. Med Sci Sports Exerc. 2018;50(7):1518-26
8. Nutr Hosp. 2026 Feb 16. doi: 10.20960/nh.06323. Online ahead of print.
9. Rev Andal MedDeporte 2011;4(4):167-74
10. J Acad Nutr Diet2022;122(9):A25
11. Med Sci Sports Exerc. 2013;45(11):2130-44

Andrew Hamilton

Latest Issue

Subscribe Today

Newsletter Sign Up
Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up

Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue

Keep up with latest sports science research and apply it to maximize performance
Today you have the chance to join a group of athletes, and sports coaches/trainers who all have something special in common...
They use the latest research to improve performance for themselves and their clients - both athletes and sports teams - with help from global specialists in the fields of sports science, sports medicine and sports psychology.
They do this by reading Sports Performance Bulletin, an easy-to-digest but serious-minded journal dedicated to high performance sports. SPB offers a wealth of information and insight into the latest research, in an easily-accessible and understood format, along with a wealth of practical recommendations.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Performance Bulletin helps dedicated endurance athletes improve their performance. Sense-checking the latest sports science research, and sourcing evidence and case studies to support findings, Sports Performance Bulletin turns proven insights into easily digestible practical advice. Supporting athletes, coaches and professionals who wish to ensure their guidance and programmes are kept right up to date and based on credible science.