You are viewing 1 of your 1 free articles. For unlimited access take a risk-free trial
Breathe easy: mouth, nose or both?
Does a having clear nose help with breathing and performance during exercise and if so, how? SPB looks at some fascinating new evidence

Nasal dilator devices such as the ‘Turbine’, which is inserted into the nasal passages, and ‘Breathe Right’, which consists of strips placed on the exterior of the nose have become increasingly popular among cyclists, runners and triathletes and (see figure 1). These devices are claimed to work by widening the nasal passage, which helps to increase and ease of airflow through the nostrils into the windpipe and lungs. In theory, this means less work for the diaphragm muscles and therefore more energy available to the working muscles. But research conducted so far on external nasal dilators has been rather inconclusive.
Nasal air flow research
In a previous 2016 study, which we reported on here at SPB, Aussie researchers studied the effects of external and internal nasal dilation devices on cycling economy (how efficiently the cyclists were able to use oxygen in their muscles to cover distance) and also 20km time trial performance(1). Fifteen trained cyclists completed three exercise sessions, each consisting of a 15-minute standardised warm up followed by a 20km cycling time trial while wearing either Breathe Right external nasal strips dilator, Turbine internal nasal dilator or no device (the control trial). During the warm up and time trial, the cyclists’ heart rates, muscle economy, ratings of perceived exertion, and breathing efforts were recorded and compared. The 20km time trial average power outputs were also compared to see whether either of the devices offered any performance advantage. The findings were pretty clear cut; there were no differences in time trial performance as evidenced by the power outputs, which averaged 270 watts for the Breathe Right trial, 271 watts for the Turbine trial and 272 watts with no device worn (control trial). In addition, there were no advantages in terms of cycling economy when wearing either of the nasal dilation devices.
Although there’s been little subsequent research into this topic, a subsequent 2021 study carried out a systematic review and meta-analysis (where all the data from previous studies is pooled and analyzed to generate more robust conclusions) into the benefits or otherwise of devices to enhance nasal breathing(2). Focussing exclusively on nasal strip use during exercise, this study looked at prior data from 19 studies and concluded that external nasal dilator strips showed no improvement in VO2max, heart rate or perceived exertion in healthy individuals during exercise. Just to confuse matters however, another systematic review and meta-analysis study carried out the followed year also looked at nasal strip use during exercise(3). Analyzing the findings from 11 previous studies, this review concluded that there was a small difference in favour of nasal dilators when compared to placebo for maximal oxygen uptake and rating of perceived exertion. The caveat however was that the certainty of the evidence was very low, meaning that more research would be needed to provide conclusive evidence for a benefit.
Figure 1: The ‘Turbine’ and nasal strips for nasal dilation during exercise

Brand new research
In the past three years, there’s been very little further research into this topic, but now a team of Swedish researchers from the University of Gothenburg have carried out a fascinating new study(4). Published in the journal ‘Frontiers in Physiology’, this study investigated whether the nasal contribution to airflow during oronasal breathing influences performance in well-trained, endurance athletes. Specifically, the researchers wanted to discover whether nasal decongestion during oronasal breathing enhances ventilatory (breathing) efficiency and if so, whether that could improve time-to-exhaustion (TTE), maximal oxygen uptake (VO2max), and maximum power output (Wmax), as compared to oral-only (mouth-only) breathing. They also sought to establish whether any benefits from improved nasal flow are exercise-intensity dependent and whether any observed effects apply equally to both male and female athletes.
What they did
Twelve well-trained, male cyclists and triathletes in the age range of 19–48 years were recruited from the Gothenburg region of Sweden. These athletes were aerobically very fit (maximum oxygen uptake capacities [VO2max] averaging 67.2mL/kg/min) and all the participants had prior experience in competitive cycling at the regional, national or elite level with typically 10 years of competition history. Following assessments for body composition (using highly accurate DXA technology), and physiological testing to calculate each participant’s maximal workload (Wmax - used to individualize the experimental protocol) and a familiarization trial in order to become accustomed with the maximal test procedures, the athletes were also screened by an ear, nose, and throat physician to check for any significant anatomical abnormalities that might affect oral or nasal breathing (there were none).
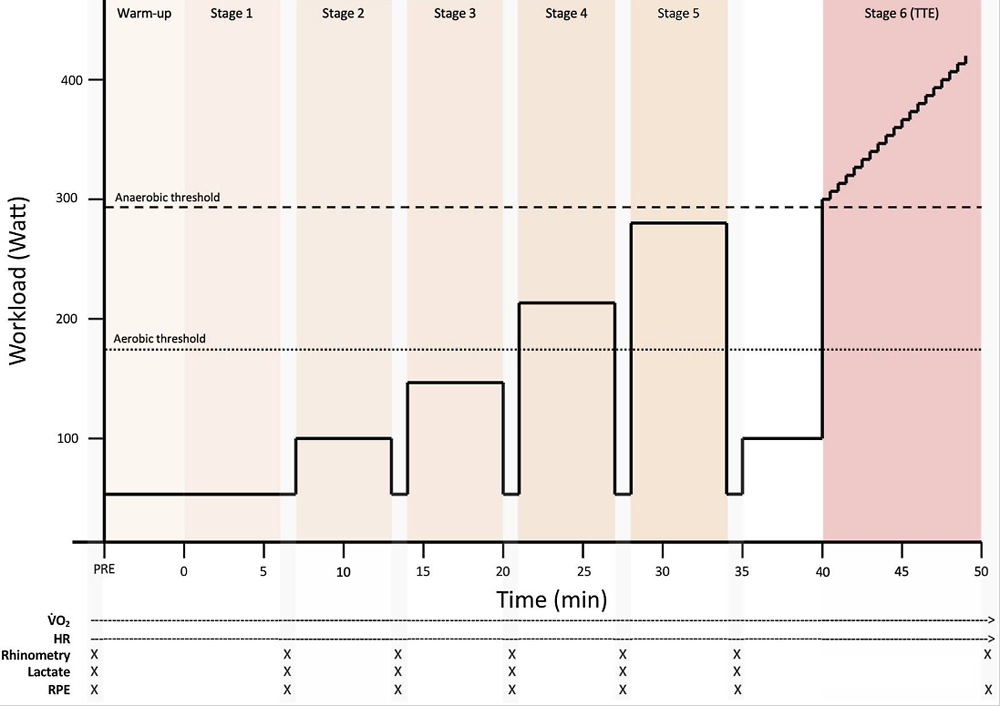
There then followed three experimental trials conducted in randomized order on three separate occasions each separated by at least four days. Each trial protocol was identical (see figure 2), consisting of five x 6-minute submaximal steady-state levels (50 watts and 100 watts at 50 rpm for the first two stages, followed by 40%, 58%, and 75% of each athlete’s individual Wmax at 80 rpm). The final stage of each trial concluded, concluding with a time-to-exhaustion (TTE) test where the power output required by the cyclists was increased incrementally by 10 watts each minute. The only difference between these three trials was how the athletes breathed during the trial. These three conditions were as follows:
· Oral-only breathing (ie through the mouth only), with the nose occluded using a nose clip.
· Oronasal breathing, where the athletes were free to breathe normally through the mouth and nose.
· Enhanced oronasal breathing following nasal decongestion. In this trial, the athletes were administered a nasal decongestant called oxymetazoline, with two sprays in each nostril 10 minutes before exercise onset to reduce congestion of the nasal mucosa and maximize nasal airflow (while still being allowed to also breathe through the mouth)
During all three trials, measures of oxygen uptake, lactate, heart rate, perceived exertion and nasal airflow were monitored throughout.
Figure 2: Experimental trial protocol for each of the three breathing trials
Related Files
What they found
When the data from the three trials was analyzed and compared, a number of findings emerged:
· Breathing and air flow - there were no significant differences between the three breathing modes (oral only, oronasal, and enhanced/maximal oronasal in terms of respiration rate (breaths per minute) or volume of air breathed per minute.
· Physiological performance – as above, there were no difference between the three breathing modes in terms of heart rates, maximum oxygen uptake and maximum power generated in the TTE test.
· Time to exhaustion test – this is where things got interesting; when the athletes used either oronasal or enhanced (decongested) oronasal breathing, they managed 2.8% and 4.2% longer respectively in the TTE test. While this gain was just a little too small to meet the strict criteria for statistical significance, a further statistical analysis using something called Cohen’s test yielded an ‘effect size’ of 0.19–0.28. This equates to an impact classed as just above negligible and below medium. In plain English, it’s likely there was a small but real effect, and that if the study had used larger numbers of athletes, the results would have met the strict statistical significance criteria.
· Average lactate levels – another interesting finding was that the average blood lactate level was significantly lower at the end of the TTE test in the oral-only breathing condition (9.12mmol/L), as compared with the oronasal (9.83mmol/L) and oronasal/decongested (9.81mmol) conditions. Put simply, when the athletes performed this maximal task to exhaustion, oral-only breathing seemed to lower lactate accumulation, suggesting less fatigue.
Practical implications for athletes
Let’s tease out the implications of these findings for athletes. In short, does the way you breathe, or increasing nasal airflow really help with performance? Looking at the data, it seems that when performing a prolonged bout of exercise at moderate to hard exercise intensity, improved nasal airflow in the oronasal and oronasal/enhcanced conditions may help sustain endurance performance, albeit providing only slight benefits. However, when the hammer is down and you are working to near exhaustion at maximal effort (eg in a prolonged sprint for the finish line or when doing hard intervals), an oral-only breathing strategy seems to reduce lactate accumulation. On reflection, many athletes may find that this is what seems to happen automatically anyway - ie breathing through the mouth and nose simultaneously during low-moderate intensity exercise, but resorting to mainly oral breathing when exercise intensity becomes very high.
A main take-home message seems to be that for athletes undertaking longer-distance endurance events, good nasal airflow is something that may help performance – or at the very least, it’s undesirable to train or compete with a blocked up nose! In practical terms, simply ensuring that you give your nose a good blow before beginning might not be bad advice. For athletes who sometimes feel that the nasal airways aren’t always free flowing (eg those suffering from allergies or colds that result in stuffy noses), a nasal breathing device or a nasal decongestant may well help. Be aware though that if you are competing under WADA rules, the use of certain nasal decongestants may fall foul of the regulations. Below are some up-to-date guidelines, but if in doubt, always check first!
|
Substance |
Banned in competition? |
Key details |
|
Pseudoephedrine (e.g., Sudafed oral tablets) |
Yes (threshold-based) |
Banned if urine concentration exceeds 150μg/mL. Oral forms can accumulate to risky levels; topical/nasal sprays are generally safer but still require caution. |
|
Phenylephrine (e.g., many nasal sprays like Neo-Synephrine) |
No (monitored) |
On WADA’s Monitoring Program for potential future prohibition; no current ban, even in-competition. |
|
Oxymetazoline (e.g., Afrin nasal spray) |
No (specified exemption) |
Allowed for nasal use within licensed doses and therapeutic indications (e.g., short-term congestion relief). |
|
Xylometazoline (e.g., Otrivin nasal spray) |
No (specified exemption) |
Allowed for nasal use within licensed doses and therapeutic indications. |
|
Ephedrine (sometimes in combo decongestants) |
Yes (threshold-based) |
Banned if urine concentration exceeds 10μg/mL. Avoid entirely if possible. |
References
1. J Sci Med Sport. 2016 Sep 1. pii: S1440-2440(16)30161-X
2. Eur Arch Otorhinolaryngol. 2021 May;278(5):1307-1320
3. J Sports Sci. 2022 Oct;40(20):2315-2326
4. Front Physiol. 2025 Sep 24:16:1654725. doi: 10.3389/fphys.2025.1654725. eCollection 2025

Andrew Hamilton

Latest Issue

Subscribe Today

Newsletter Sign Up
Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up

Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue

Keep up with latest sports science research and apply it to maximize performance
Today you have the chance to join a group of athletes, and sports coaches/trainers who all have something special in common...
They use the latest research to improve performance for themselves and their clients - both athletes and sports teams - with help from global specialists in the fields of sports science, sports medicine and sports psychology.
They do this by reading Sports Performance Bulletin, an easy-to-digest but serious-minded journal dedicated to high performance sports. SPB offers a wealth of information and insight into the latest research, in an easily-accessible and understood format, along with a wealth of practical recommendations.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Performance Bulletin helps dedicated endurance athletes improve their performance. Sense-checking the latest sports science research, and sourcing evidence and case studies to support findings, Sports Performance Bulletin turns proven insights into easily digestible practical advice. Supporting athletes, coaches and professionals who wish to ensure their guidance and programmes are kept right up to date and based on credible science.